
Why Treatment Is Needed
Untreated coarctation can lead to:
- Severe or resistant hypertension
- Heart failure
- Stroke or aortic rupture
- Early coronary artery disease
- Reduced life expectancy
Early correction significantly improves survival and blood pressure control.
Who Is Suitable for Stenting?
- Adolescents and adults with native coarctation
- Recurrent coarctation after surgery or balloon angioplasty
- Significant pressure gradient (>20 mmHg) across narrowing
- Hypertension related to coarctation
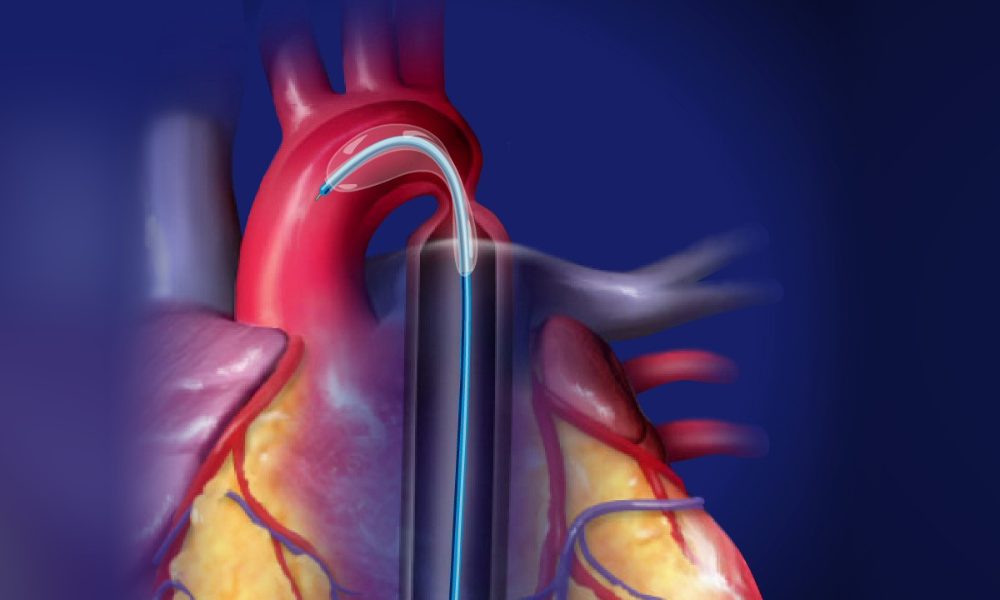
How Coarctation Stenting Is Performed
- Access via femoral artery
- Angiography to define anatomy
- Balloon dilatation of narrowed segment
- Placement of a covered or bare-metal stent
- Post-dilatation to optimize aortic diameter
- ⏱ Procedure time: 60–90 minutes
- 🏥 Hospital stay: 2–3 days
Types of Stents Used
- Covered stents (preferred): Reduce risk of aortic rupture or aneurysm
- Bare-metal stents: Used in selected anatomies
Benefits of Stenting
- Immediate reduction in pressure gradient
- Improved blood pressure control
- Avoids open-heart surgery
- Short recovery time
- Excellent long-term outcomes
Safety & Outcomes
- High procedural success (>95%) in experienced centers
- Low complication rates
- Long-term patency with regular follow-up
- Some patients may still require antihypertensive therapy
Post-Procedure Care
- Blood pressure monitoring and medications
- Echocardiography and CT/MR angiography follow-up
- Avoid heavy exertion initially
- Endocarditis prevention measures
Special Considerations
- Lifelong BP monitoring is essential
- Bicuspid aortic valve
- Cerebral aneurysms
- Pregnancy planning in women with repaired coarctation
Screening for associated conditions:
Indian Context
- Many patients present late with hypertension
- Stenting widely available in tertiary congenital heart centers
- Covered stents commonly preferred for safety
